Institutional governance, data ownership, and stakeholders’ engagement, and resource mobilization
Step 1
Summary
Although nearly all LMICs could benefit from an SMSS, implementing one can be challenging and requires that several prerequisites are satisfied. The continuous nature of an SMSS requires a medium- to long-term commitment and planning. Planning the system to ensure that it will be useful and relevant at addressing the country’s health data needs is essential. Obtaining buy-in from high level government leadership is an initial step that can greatly facilitate subsequent steps and ensure a successful engagement of all stakeholders. In addition, there are important implications related to institutional capacity, feasibility, financial and human resources, and sustainability. We outline below key considerations, including deciding on institutional leadership, data ownership, and stakeholders’ engagement. Budget and financing considerations are also examined at this stage.
Institutional Leadership
Leadership from the government, through a designated government institution, is essential to undertake all required steps and ensure accountability effectively. Strong leadership is required to build the credibility needed for government and stakeholders to buy into and use official statistics. Furthermore, leadership from a government institution will facilitate linkage or integration with existing government data systems, such as the CRVS or the HMIS, the ability to convene key stakeholders, and to abide by government-established guidelines and rules. Given the goal of data and statistical production, government-mandated institutions must be first engaged to discuss the content, scope, and responsibilities.
In many African countries, national statistical offices have such mandate. However, the system’s focus on health indicators and potentially its extension to other areas such as disease surveillance may mean that the Ministry of Health should have this mandate instead depending on its capacity to successfully undertake continuous heavy national data collection. Many countries have also established national public health institutes that are mandated to conduct health surveillance activities within the country and generate evidence for health-related decision-making. These institutes often lead the implementation of sero-surveillance surveys or other national health surveys such as the malaria indicator surveys and the HIV/AIDS surveys. Public health institutes or ministries of health can serve as an ideal home institution for the surveillance system, where linkage can be established with other government institutions or departments. In some cases, partnership between the national institute of statistics, civil registration authorities, and an existing public institute can be established with clear division of labor and leadership to avoid conflicts in the long run. An established institutional lead of the SMSS will establish a clear line of accountability for the system.
Data Ownership
Institutional leadership will often define who ‘owns’ the data derived from the SMSS system. Whichever ministry or agency/institute is the owner of the data, however, annual reports and deidentified aggregated should be freely made available to the public. In addition, the Ministry of Health will need unrestricted access to the raw data sets on a continuous basis to fulfill its public health functions such as detecting outbreaks and health planning down to the district and sub-district levels. In no case will agencies with access to these data, regardless of ownership status, be able to publish information about individuals to the public. Permissions should follow “meaningful use” guidelines, consistent with the country’s rules.
Stakeholder Engagement
Knowledge about birth and death events in the population, or use of this information, is the responsibility of many government ministries, agencies and institutions. In order to design an SMMS system that benefits these stakeholders, collaboration and co-creation is required. Representatives of the following agencies are typically included in the design process for the SMSS: Bureau of Statistics, Ministry of Health (including hospitals and public health institutes), Civil Registration and Vital Statistics, Mortuary Services, Ambulance Services, Police and Fire, and local government. Representatives from other agencies should be considered as applicable in each country depending on who needs to know or use this information and/or who is engaged in collecting these data. Consider engaging each agency independently to gauge interest, and then bring the relevant agencies together for a series of co-creation events to design the system and adjust the design periodically based on experience (i.e., adaptive management). A comprehensive and successful stakeholder engagement can be achieved by first mapping and organizing all stakeholders based on their stake in the SMSS in terms of data production, analysis, use and dissemination. The position of each stakeholder can be determined using a two-by-two matrix based on the degree of interest (low, high) and power (low, high). The type of engagement can then be determined based on the quadrant in which the stakeholder falls. Stakeholders with high interest and power are key players and must be closely involved in the development, implementation, and dissemination activities of the SMSS. Stakeholders with high interest and low power will need to be kept informed and involved in advocacy efforts. Stakeholders with low interest but high power can potentially be opposed to the system. They must be kept informed and their views acknowledged. Stakeholders with low interest and power may only require minimal engagement. Additional resources can be accessed here.
Resource Mobilization
The expected costs for an SMSS (based on nominal 2020 values for a system covering about a population of about one million in a country like Mozambique with about 30 million people) is approximately $2 million dollars to start up the SMSS system and about $1 million in recurrent costs each year after start-up. Below is the breakdown of start-up and recurrent costs of the Mozambique COMSA/SIS-COVE system. In addition to Mozambique Government funding, funds also were raised from foundations, bi-lateral donors, and the Global Fund. See the linked article below, “*Implementing the Countrywide Mortality Surveillance in Action in Mozambique: How Much Did It Cost? An original research article from the 2023 COMSA supplement in The American Journal of Tropical Medicine and Hygiene.
Table 1: Example Start-up Fixed Costs for the COMSA/SIS-COVE Project 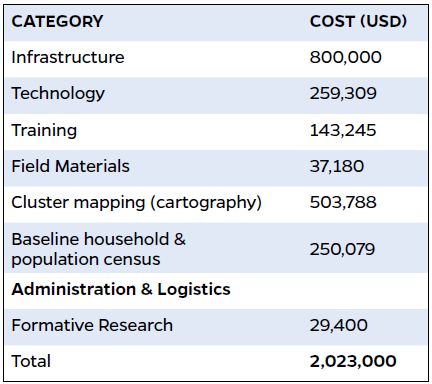
Table 2: Example: Recurrent Costs for the COMSA/SISCOVE Project 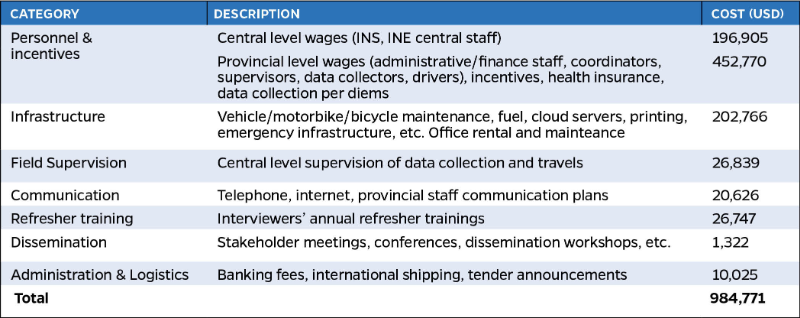
To Learn More:
-
*Mozambique Sample Vital Statistics System: Filling the Gaps for Mortality Data A commentary from the 2023 COMSA supplement in The American Journal of Tropical Medicine and Hygiene.
-
*Implementing the Countrywide Mortality Surveillance in Action in Mozambique: How Much Did It Cost? An original research article from the 2023 COMSA supplement in The American Journal of Tropical Medicine and Hygiene.
-
*From External to Local: Opportunities and Lessons Learned from Transitioning COMSA-Mozambique An original research article from the 2023 COMSA supplement in The American Journal of Tropical Medicine and Hygiene.
| Last updated |
|---|
| May 12, 2026 |