Routine Data Collection and Transfer
Step 10
Community data collectors routinely visit the households in their cluster to collect information about pregnancies, pregnancy outcomes and deaths. Verbal autopsy data collectors revisit the homes after a mourning period to conduct verbal autopsy interviews. Other project team members conduct data quality checks and cleaning. These steps require a system of electronic data capture, transfer and management.
Community Surveillance
Community surveillance involves the continuous collection of data on vital events, including pregnancies, pregnancy outcomes and deaths, and follow-up to families where deaths are identified for verbal and social autopsy interviews. After the baseline mapping and listing of household population, described in step 9, are complete, the trained community surveillance agents (CSA) should visit all households within their clusters every 2-3 months and record information about new vital events using their project-assigned smartphones. If new households appear in the cluster, they are also registered and consented into the surveillance. As described in step 6, data collected in the community are uploaded to the project servers. This allows all new deaths or stillbirths to be automatically populated on the dashboard and assigned a death ID. The VASA supervisors then schedule them for a follow-up visit at which time a VASA questionnaire is completed. Such visits are scheduled for after approximately a month following the death to allow time for mourning. The supervisor can attempt to schedule several VASA visits around the same time and location to save resources and use staff time efficiently. It can be helpful to contact the family by phone to confirm that they are available on the appointed date. On the dashboard, at each stage of the process, the status of the reported death can be tracked from when it’s reported to when the VASA interview is scheduled, until finally when the VASA interview is completed. This assures that all death events are followed up to complete the VASA interviews. A small number of families will be unreachable, possibly because they have moved, and some families will refuse to complete the interview. In these cases, the VASA interview visit is still considered completed and the case considered as a lost to follow up or non-response.
Supervision of the Community Data Collection
The supervisors of CSAs must maintain monthly communication with the CSAs via phone calls or SMS on their routine surveillance activities, and provide them with the necessary resources and support. These supervisors are also the VASA data collectors and can meet with the CSA during their VASA interview visits in the cluster. A progress monitoring sheet may be implemented to document contact with CSAs and their work progress. Furthermore, the supervisors have access to the data reported by the CSAs through the Dashboard. They should review these ahead of contacting the CSAs to provide them with adequate feedback.
The supervisors must also routinely survey a sample of the houses to ascertain the completeness of the data reported. At the end of every year (at twelve-month intervals), a data recapture exercise must be completed by tasking the CSAs to visit every household within their clusters and collect data on events that have occurred in the past twelve months. This exercise will help improve the completeness of the community data reporting but also help understand patterns of missing events, identify well performing CSAs and provide an opportunity to refine the community surveillance. Depending on how well the CSAs are performing in capturing the vital events, such data capture activity may be planned every six months.
In addition to the annual data recapture, a population update and data assessment activity should be planned every 2-3 years by conducting a complete census of all clusters by an external team. These activities are described in step 12.
VASA Data Supervision
The VASA teams are based in each province and are the first point of contact with community data collectors. In addition to administering the VASA questionnaire, they also supervise and train community data collectors whenever required. Routine reports are generated on the following and discussed at weekly and monthly meetings with the provincial coordinator and the central level focal points:
- Number of VASA interviewers done by each VASA data collector and outcome of the VASA visit.
- Frequency of contact between the VASA staff and the data collectors they supervise.
Data Review and Quality Assurance
A routine progress report of work completed is generated for each cluster and discussed at both the central and provincial levels. The central data team monitors the number of events reported monthly, and a 3-month cumulative report is then used to determine which community data collectors are active. Inactivity can also indicate issues with technology, such as phone functionality or connectivity.
The VASA reports show the number of death events and the progress of VASA data collection. A key indicator is the monthly number of completed VASA interviews and the total number of pending VASA interviews. If pending VASA interviews grow over time, this can indicate the team is falling behind and may need support.
Data Repository
As described in step 6, all data collected by the CSAs and VASA data collectors, are managed on the analysis portal. Both raw and clean data are retained. The clean data is processed into a format that is user friendly by the analysis team.
Data Flow
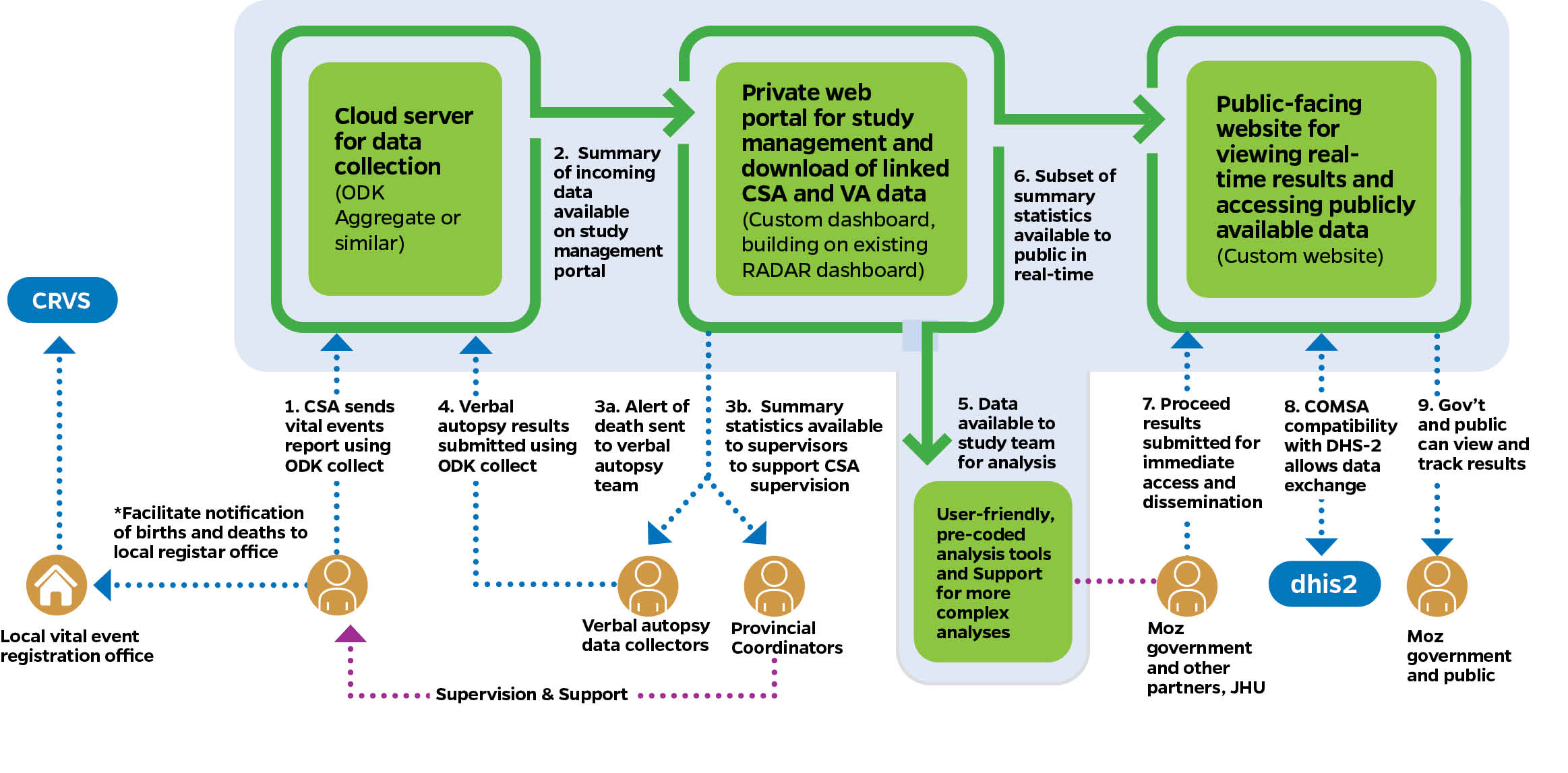
Data captured at the community level is transferred electronically to a cloud server specifically set up for the data collection (see step 6 on digital solution and IT). Similarly, VASA data collected are directly uploaded to the cloud server. A separate server may be set up for data processing, cleaning, and analysis. The diagram above shows the data collection flow used in the COMSA/SIS-COVE SMSS, which will be similar to systems in other settings. Details about how data collection is implemented are described below.
Data Linkage/Integration
The development and implementation of an SMSS must consider existing mortality data systems within the country and be designed in a way that links or integrates with them. The two essential existing systems to account for are the CRVS and the RHIS. The SMSS will collect sample-based representative and individual level data on population, births, and deaths. These vital events are also collected, in varied forms, by the CRVS and RHIS. Linkage or integration between the SMSS and CRVS and RHIS can be implemented in several ways:
-
Given an SMSS aims for rigorous and sampled-based mortality data, statistics produced by the SMSS can be used to assess the quality and completeness of the CRVS and the RHIS mortality estimates and therefore serve as source of data for monitoring progress in the scale-up of CRVS. For RHIS, SMSS data will help understand patterns of deaths at health facility levels and health facility use. Social autopsy data can help uncover quality of care issues within the health system. Thus, an ecological linking of the SMSS, CRVS, and RHIS data at the provincial level (domains of representativeness levels) will help with mortality data triangulation at this level and serves as stronger sources for policy and program decision making and resource allocation. Events data collected by the SMSS can be directly transferred to the civil registration unit and help improve the completeness of their registration, at least within the SMSS clusters. In this case, the SMSS may incorporate modules or be designed in a way that is interoperable with the CRVS system, allowing easy electronic transfer of data and notification of events. This approach is being tested with COMSA/SIS-COVE in Mozambique.
-
Once the SMSS is functional, approaches for using the system to facilitate the scale-up of the CRVS at the district and provincial level can be tested. A linkage between the SMSS clusters and registration posts can be established. The Mozambique SIS-COVE has pilot tested the use of its community workers to complete CRVS forms for births and deaths and facilitate registration within districts in a province. Such approach can be further reviewed within each context, tested, and possibly scaled up.
-
The SMSS cause of death data is an adequate source of data for assessing differences in cause of death structure between community and facility deaths and comparison of verbal-autopsy derived cause of death with medically certified cause of death (MCCOD). Such analysis and triangulation will draw further attention to the status of the MCCOD and develop strategies for its improvement. In areas where facility use is high and most deaths occur in facilities, MCCOD can become a reliable source for cause of death data.
-
Finally, mortality data output from SMSS can be also housed within the RHIS system (e.g. DHIS-2) to promote comparison and use. A module in DHIS-2 has been developed in Mozambique within which several indicators from SIS-COVE data are included.
To Learn More:
World Health Organization Verbal Autopsy Tool (2022) COMSA-SiS-COVE Protocol and Data Collection Tools Verbal and Social Autopsy Toolkit • Produced by Johns Hopkins University’s Institute for International Programs.